The period between the First and Second World Wars saw the development of warfare concepts not previously seen and other concepts that were, at most, still in their infancy at the end of World War I. The notion of amphibious warfare was not new but certainly had not been advanced as a modern technique. The United States Marine Corps led the development of amphibious warfare doctrine and equipment. One piece of the overall doctrine that needed to be established and refined was medical support for amphibious warfare, which was the responsibility of Navy medical staff assigned to support the Marines. As such, a relatively small group of physicians networked to create workable medical support doctrine for amphibious warfare and contributed to the ability of U.S. forces to undertake amphibious operations when America entered World War II.
Medicine and warfare have been bound together for millennia, almost as long as there have been organized militaries and individuals identified as doctors. Hippocrates advised the aspiring iatros (physicians/surgeons) that, if they wanted to be surgeons, they should follow the army.1 The Imperial Roman Army had a well organized and efficient medical service that set standards not exceeded until relatively modern times.2 While the general principles of military medical care and the organization of a military medical service have remained constant, in many ways, the details of this care must adapt to the circumstances of each campaign. The physical environment, the weapons employed, and the technology of transport are as important as the advances in medical care. As such, amphibious warfare requires that medical doctrine be tailored to fit the unique environment, weapons, and transport vehicles used in this mode of warfare.
Once the Marines had identified a role for which they were particularly suited, and one for which the Army wanted no part, the Corps had to develop the appropriate doctrine.3 Military doctrine provides a road map for planning and carrying out a set of operations to achieve a given objective. At a minimum, doctrine provides a list of tasks, both planning and operational, that must be accomplished and usually defines who is responsible for those actions. Doctrine gives all of the participants a common starting point and vocabulary, thereby allowing for coordinated planning and execution.
Although amphibious operations have taken place as far back in history as the Persian invasions of Greece, there are no large-scale, successful recent amphibious assaults to use as a model. The only major amphibious assaults in modern warfare can be seen in the British and French efforts at Gallipoli in 1915 and the smaller German assaults on three Baltic islands in 1917. The latter effort, against an ill-prepared and poorly led force, was successful, while the former against a prepared and well-led force was a disaster.
The primary model for the Marines came from Gallipoli, which was studied extensively as a lesson in what not to do.4 The German assault on the Baltic Islands in 1917 could also be considered; however, the scale and special circumstances of that campaign, where Russian defenders were, along with the rest of the Russian military, in a partial state of collapse following the revolution, meant the Baltic as- sault held few lessons for the Marines. A great deal has been written about the development of Marine Corps doctrine for amphibious assaults during the interwar period, and also for the development of key equipment for amphibious warfare, such as the Higgins boat and amphibious tractor (AMTRAC/Alligator).5 A considerable amount of this development and procurement occurred in spite of, rather than because of, official channels. Warfare is not only about those who pull triggers, the Marines charging across the beach, the big ships providing gunfire support, or the aircraft strafing troops and isolating the beachhead. Take, for example, a well-worn military aphorism that says “amateurs talk tactics, professionals talk logistics.”
One general category of logistics includes medical support, which consists of two main areas: treatment of the wounded and sick; and measures taken to prevent the force from becoming sick (i.e., preventative medicine). Just as other aspects of a military operation must be tailored to the specific circumstances, so too must medical support. Medical support has the same requirement for doctrine as any other aspect of a military operation, and therefore as the Marines developed doctrine for amphibious assault, there was a need for a concomitant medical doctrine for amphibious assault, or more generally all aspects of amphibious warfare, to be developed.
On many levels, line officers tend to give thought to medical support only when it is absent. It was (and often still is) expected that “the docs” would be present when and where needed with the equipment and personnel to provide for the medical requirements of the force.6 In the case of the Marine Corps, this area of potential miscommunication was exacerbated by the fact that the medical personnel who took care of Marines were all Navy personnel, and they were under the administrative control of the Navy through the Bureau of Medicine and Surgery (BUMED) and the Bureau of Naval Personnel (BUPERS). This could, and frequently did, lend credence to the concept that receiving adequate medical support where and when needed was “the Navy’s problem.” This was certainly the case with the development of amphibious doctrine by the Marines and Navy.
During the 1920s and the early 1930s, Marines were not researching the issue of medical support, nor was medical support for amphibious warfare being analyzed by BUMED or the Navy line.7 The Navy emphasized instead building and modernizing the fleet during times of financial stringency and strong pacifistic and isolationist sentiments. At the same time, BUMED worked continually to meet the needs of naval hospitals and ships in the face of personnel shortages. The Marines’ needs ranked lower on the priority list, and issues of medical support for potential amphibious operations lower still.
When outlining the basics of amphibious operations and amphibious assaults, medical support in this environment is neither simple nor intuitive. Yet by the time the Corps made its first amphibious assault in August 1942 on Guadalcanal, medical planners had written doctrine for medical support, which the Navy and Marine Corps implemented and which worked. A few months later, when the Army landed in North Africa, they, in conjunction with the Navy, used the same doctrine to support those landings. Just as with other aspects of amphibious doctrine, that for medical support came as the result of analysis, experimenting, and testing. In fact, a small number of Navy doctors closely associated with the Marines, more or less without direction or sometimes without much support, made it their mission to develop the necessary doctrine. What these doctors did, in fact, had very little to do with direct medical care; their actions were less about better surgical techniques or new medications, and more about devising a system of care adapted to the particular circumstances of amphibious operations. This system encompassed organization, personnel, equipment, and a doctrinal template for planning and implementation that is still the basis for current Marine Corps medical planning. Doctors with clinical skills and experience were needed to define the parameters of what care, whether preventative or reparative, would be provided to the amphibious task force and assault force. Naval officers with experience in Marine Corps operations were needed to define the parameters of what could be done: in particular, how best to provide the physical and human infrastructure to produce the desired care within the limits imposed by the realities of an amphibious assault. The process relied on input from specialists; in the end, however, a small group of individuals with disparate skills and knowledge made the hard decisions about overall doctrine and what and who to include on the tables of equipment and personnel.
As a result of their work, appropriate medical doctrine and support was “there” when it was needed; therefore, the military analysts and historians of amphibious warfare who have examined many other aspects of doctrinal development during the interwar period have ignored medical doctrinal developments.8
This article represents the first in a three-part series that will explore how the U.S. Navy and Marine Corps established medical doctrine for amphibious warfare during the period between World War I and World War II. In many ways, doctrinal development follows the standard military planning process for any operation: (1) define the mission, (2) produce alternate plans, (3) test these plans (by experimentation or wargaming), (4) repeat these steps until a final plan is promulgated, and (5) finally analyze the plan’s success or failure to support the development of future plans. Unlike establishing doctrine and the processes for the development of equipment, creating medical doctrine became almost an informal process. Navy doctors who combined the requisite skills and operated with the Marines saw the need to create this doctrine, and established a casual network of like-minded officers working on the issue.
The use of counterfactuals in history, such as “what if ” General Robert E. Lee had won at Gettysburg or the Navy carriers had been docked at Pearl Harbor, are not usually a useful tool. In this case, however, it was valuable to ask the “what if ” of amphibious medical doctrine having been thrown together at the last minute. The Gallipoli example answers the “what-if” for our purposes. The section on Gallipoli in the Official History of the Australian Army Medical Services 1914–1918 (1930) describes in painful detail how the lack of proper planning caused vast amounts of unnecessary suffering. This analysis should also serve as a reminder to those who write military history and to those who study it that military operations work much like an arch, whereby the keystone may be the most important and visible piece but, absent all of the supporting pieces, the arch will collapse no matter how solid the keystone.
Concepts of Amphibious Warfare
Perhaps no other class of military operations illustrates Clausewitz’ maxim that “everything is very simple in war, but the simplest thing is difficult” better than amphibious warfare.9 Initially, processes appear straightforward and analogous to conventional land warfare, such as loading troops and equipment on transports (in this case ships not trains, wagons, or trucks), deliver them to the point of assault, and once an adequate bridgehead has been secured, the campaign transitions to “normal” land warfare. This superficial analysis, while not inaccurate, is woefully incomplete. Many military analysts would agree that no military operation is as complex as an amphibious assault, no other where attention to detail is as critical, and none more likely to produce large numbers of casualties so quickly.10
A basic understanding of the major issues in amphibious warfare is necessary to grasp both the overall process of amphibious warfare doctrine by the Navy and Marine Corps and the corollary issues regarding the development of medical doctrine for amphibious warfare. While the overarching amphibious doctrine and plan provides guidance for the creation of subsections or subplans, medical planners must provide accurate and appropriate input up the chain of command to ensure that their needs are integrated into the overall plan.11
An attack that achieves maximum surprise and avoids a direct assault has a higher chance of success, and is much more likely to result in fewer casualties. Unfortunately, amphibious assaults rarely achieve these conditions. These offensives almost always come from a direct frontal assault, with the force completely exposed during transport to the beach and upon the beach, thus creating the greatest potential for a large numbers of casualties in a short period of time. Unlike a land battle, transporting the wounded to treatment facilities becomes much more difficult. All wounded, even those who could normally walk to an aid station, must be transported back to a ship for the medical care provided on a beach remains limited until it is relatively free from the enemy or incoming fusillades. Once the beach is adequately safe, medical units have to be landed and made operational; such units should be as compact as practicable to conserve weight and space and their resources need to be packed in waterproof containers to prevent spoilage due to spray or submersion. Ship loading the Amphibious Task Force (ATF) presents a major planning issue in amphibious warfare. Equipment and supplies need to be packed with the requisite units, and placed in storage in the re- verse order of use, with equipment needed first on the top. Also, the assault force cannot transport the entirety of one type of equipment (or one class of personnel) in one ship, because if that ship sinks then all is lost. Failure to understand the concepts of combat and spread loading bedeviled American landings at Daiquiri, Cuba, during the Spanish-American War, and the British and Commonwealth troops at Gallipoli. In the former case, vital medical supplies were still onboard ships weeks after the landing due to lack of planning during the loading process. At Gallipoli, medical equipment and supplies were often on different ships than those carrying the medical units, which then landed with only minimal ability to perform their duties. Medical planners must understand what equipment (and personnel) will be needed, when it will be needed, and where it will be needed. Otherwise, appropriate medical care will not be available in a timely fashion.
Until the campaign transitions from an amphibious assault to a traditional land campaign, or an island is secured, transporting wounded involves significant shore-to-ship movement. This is not merely an issue of having adequate landing craft designated for the movement, but also ensuring that the wounded are transported to the appropriate ship with both the facilities and the personnel to receive the wounded but also available space for the wounded. Failure to put such a system (medical regulating) in place was one of many tragedies in the early part of the Gallipoli operation, when barges of wounded drifted from ship to ship trying to find treatment. Even when they found a vessel to offload the wounded, the receiving ship was frequently inappropriate, lacking appropriate medical spaces, personnel, and equipment.12
Some of the equipment issues particular to amphibious operations have been mentioned previously. Simplicity and minimizing the weight and volume of the equipment is important, even more so with amphibious operations than in traditional land campaigns. Equipment must be thoroughly waterproofed or packed in waterproof containers and be protected not just from moisture, but also from highly corrosive salt water. Just as the transports must be combat ready and spread loaded, equal thought and preparation must go to the equipment for a medical unit as this equipment is as liable for loss during the landing as any other.
The many factors specific to amphibious operations illustrate the need for meticulous planning, and for the medical staff to have a concept of operations and doctrine that meshes with that of the command and the operation. The Australian report on Gallipoli, and the results of Army investigations of medical failures from the Spanish-American War, demonstrate the impact of a massive failure of proper medical planning. While medical doctrine for traditional land warfare and assaults can be used as a starting point, the demands of an amphibious assault require a special and specific doctrine.
The 1920s
The 1920s represent a decade of challenge for the U.S. military, and the Marine Corps was not an exception. Although the United States had become a major force on the world stage and was more than 20 years into being an imperial power, America was turning inward. The Senate acceptance of the Versailles Treaty with the provisions for the League of Nations was defeated for a variety of reasons, both political and philosophical. The military forces that had been built up for the Great War were rapidly reduced, as Congress and the public saw no need for a permanently expanded force much above prewar levels. Huge stockpiles of everything from uniforms to ammunition sat in warehouses, with the surplus to be used before a parsimonious Congress would consider anything new. In fact, U.S. forces would be eating World War I rations and using all manner of World War I equipment when they went into action after Pearl Harbor.
With massive reductions in funding, carrying out anything more than the most necessary operations was difficult. Money for exercises was slim, and military pay during the 1920s was not competitive with the booming civilian economy. As a result, recruiting was difficult and the Marines were not able to fill even the reduced number of positions they had been allotted. The Navy had personnel shortages as well, which affected the Corps in terms of assigning medical officers and corpsmen to fill full time, as opposed to temporary or exercise only, billets. Operating on even more of a shoestring budget than usual had an effect on plans to revamp Marines as an amphibious assault force. In one respect, the Marines were fortunate. Commandant Lejeune had made the decision about the direction the Corps was going to take, stating formally in 1922: “The primary war mission of the Marine Corps is to supply a mobile force to accompany the Fleet for operations on shore in support of the Fleet. This force should be of such size, organization, armament, and equipment as may be required by the plan of naval operations.”13 Early versions of War Plan Orange (war with Japan) recognized the need to seize island advance bases. Since the Army wanted nothing to do with amphibious warfare, with the amphibious mission formally allotted to the Marines by the Joint Board, the Marines had a well-defined mission to provide a future for an independent Marine Corps even in an era of retrenchment and isolationism. As long as the Marines could operate within tight fiscal and personnel constraints, developing the amphibious force and its doctrine had been given a green light to proceed.
As noted, Lejeune had taken the Advanced Base Force concept and used it as the springboard for a Marine Corps built around the model of amphibious warfare even before he ascended to the commandancy. Immediately following the end of World War I, Lejeune assigned Major Earl “Pete” Ellis to evaluate potential Marine Corps operations against Japan in the context of an “Orange” war. Following WWI, the chances of a conflict between Great Britain and the United States faded into improbability, and Germany had been eliminated as a threat for the immediate future. The Atlantic Ocean was, so it seemed, secure. However, the Pacific Ocean and Asia still presented the potential for conflict between the United States and Japan. Military planners looked on a U.S.-Japan conflict as the most probable outcome. Civilian and general readership books, such as Walter B. Pitkin’s Must We Fight Japan? (1921) and Hector C. Bywater’s Sea-Power in the Pacific: A Study of the American-Japanese Naval Problem (1921), highlighted the fact that conflicting American and Japanese interests would lead to war.
Because the German Pacific islands north of the equator had been ceded to Japan under a League of Nations mandate, the sea lanes between Hawaii and the Philippines could be readily interdicted by the Japanese as the U.S. possessions along this route—Midway, Guam, and Wake islands—were isolated and far from any support.14 It was clear that any attempts by the United States to relieve or recapture the Philippines would require seizing advance bases on islands currently occupied by Japan. In addition, these bases would be needed to support the fleet as it advanced west in anticipation of the Mahanian (Alfred Thayer Mahan: Influential U.S. Navy admiral, historian, and geostrategist in the late 19th century) clash of battle fleets to take place near Japan. Hence, the study by Major Ellis was presented in 1921. The provisions of the treaty from the Washington Naval Conference in 1922 where the United States and Japan agreed to forgo fortifying almost all Pacific island bases meant that, in case of conflict, most if not all U.S. possessions west of Hawaii would be over-run, thus increasing the need for a plan to seize new or to retrieve old bases.
Ellis’ Advance Base Operations in Micronesia (FMFM 12-46), as detailed and prescient as it was, made no mention of casualties or medical treatment of casualties.15 He would not be the first Marine Corps planner to ignore this issue; most Marine officers saw the issue of medical care as “the Navy’s problem” and, furthermore, felt out of their depth when considering medical issues. This is not to say that the issue of casualties was completely ignored in the war planning process. Captain D. N. Carpenter, Medical Corps, USN, who was a medical planner, outlined the needs for hospital beds in an Orange (Japan) war scenario to Captain H. R. Stanford Civil Engineering Corps, USN, who was a civil engineering officer. Hospital bed needs were estimated at 19,262, however, Carpenter noted that hospitalization (initially) for the Advanced Base Force would be on class A hospital ships, but no estimate was given for the number of ships required.16
Fortunately, there were Navy and Marine officers who were aware of the gap between the doctrine of the new Marine Corps and the medical establishment and the doctrine that would support it. Between July 1922 and January 1923, Major S. N. Raynor, USMC, published a six-part series in the United States Naval Medical Bulletin entitled “The Functions and Organization of Medical Corps Units Serving with the Marine Corps in the Field.”17 The editors explained the rationale behind this series of articles in the introduction to the first part:
The writer has undertaken to prepare for the UNITED STATES NAVAL MEDICAL BULLETIN a series of articles dealing with the functions and suggested organization of Medical Corps units serving with the Marine Corps in the field. Up to the present time there has been no special organization for that service. If the necessity for such special organization can be demonstrated, the quo animo of this series shall have been attained.18
Furthermore, the editors informed the readers that Major Raynor had created an appropriate correspondence course through the Marine Corps schools at Quantico, Virginia, and the surgeon general was “desirous” that all medical officers available for service with the Marines take this course.19 Since a brief article had appeared in this same journal at the beginning of 1922 announcing this course and explaining the rationale behind it, the emphasis and strong endorsement implies that the number of medical officers taking the course must have been below expectations and goals.20
At the beginning of part two of this series, the editors elaborated further upon the reasoning behind the series. They detailed how service ashore with the Marines created a different environment with different challenges than working aboard ship or in a hospital and that, to properly function in this setting, the medical officer had to be appropriately trained and educated. This training and education had to include not only the specifics of the duties as a medical officer, but also how to function personally and as a staff officer within the military (as opposed to naval) milieu.21
In the article, Major Raynor set forth the notional organization of a Marine brigade with its components, both medical and line.22 This organization was essentially a copy of an Army unit. Likewise, the notional table of equipment (T/E) that Major Raynor described was also a copy of the Army T/E. Outlines of the requirements of the administrative order (operations order or “OPORD” in today’s vernacular) and examples of how and with whom to interface on the staff to accomplish tasks were also detailed in the article. Overall, this relatively short article—a distillation of the correspondence course—still represented a giant leap forward when compared to the Navy’s Landing-Force Manual.23 The latter is extremely limited when discussing medical issues, and seems suitable only for addressing the conduct of operations with a relatively small number of sailors detached from a ship to form a landing party.
Although Major Raynor and the Navy medical establishment had made a necessary start to developing doctrine for Navy medical support of the Marines, a critical and glaring hole in this doctrine became obvious: there was no mention of amphibious operations. The concepts of the duties of a senior medical staff officer presented in the article, and development of the medical annex to the overall plan and how to prepare it, were applicable to any operation. However, the very specific issues of amphibious assault were completely ignored. And just as operating with the Marines is very different from operating on a ship, so too is the medical task of an amphibious assault different from that of a “standard” land campaign, which had not yet been articulated.
Almost simultaneously with Major Raynor’s article, the United States Navy Medical Bulletin published an article by Lieutenant Commander William L. Mann Jr., Medical Corps, USN. A highly detailed article dealing primarily with the preventive medicine issues of Marine forces ashore, this piece was intended to serve as a “how-to” guide, rather than as a conceptual leap.24 As with Major Raynor, Lieutenant Commander Mann was dealing with an established land campaign, and issues concerning amphibious assault were not mentioned at all. Similarly, Mann based his organization and planning on Army models. It would not be until 1927 that the Navy would collect and expand upon the articles and publish this compendium as a textbook. Even if many of the concepts and diagrams were essentially copied from Army manuals, his illustrations as well as his text provide the most useful practical guide for a medical officer assigned to the Marines produced to date (see figures 1–4).
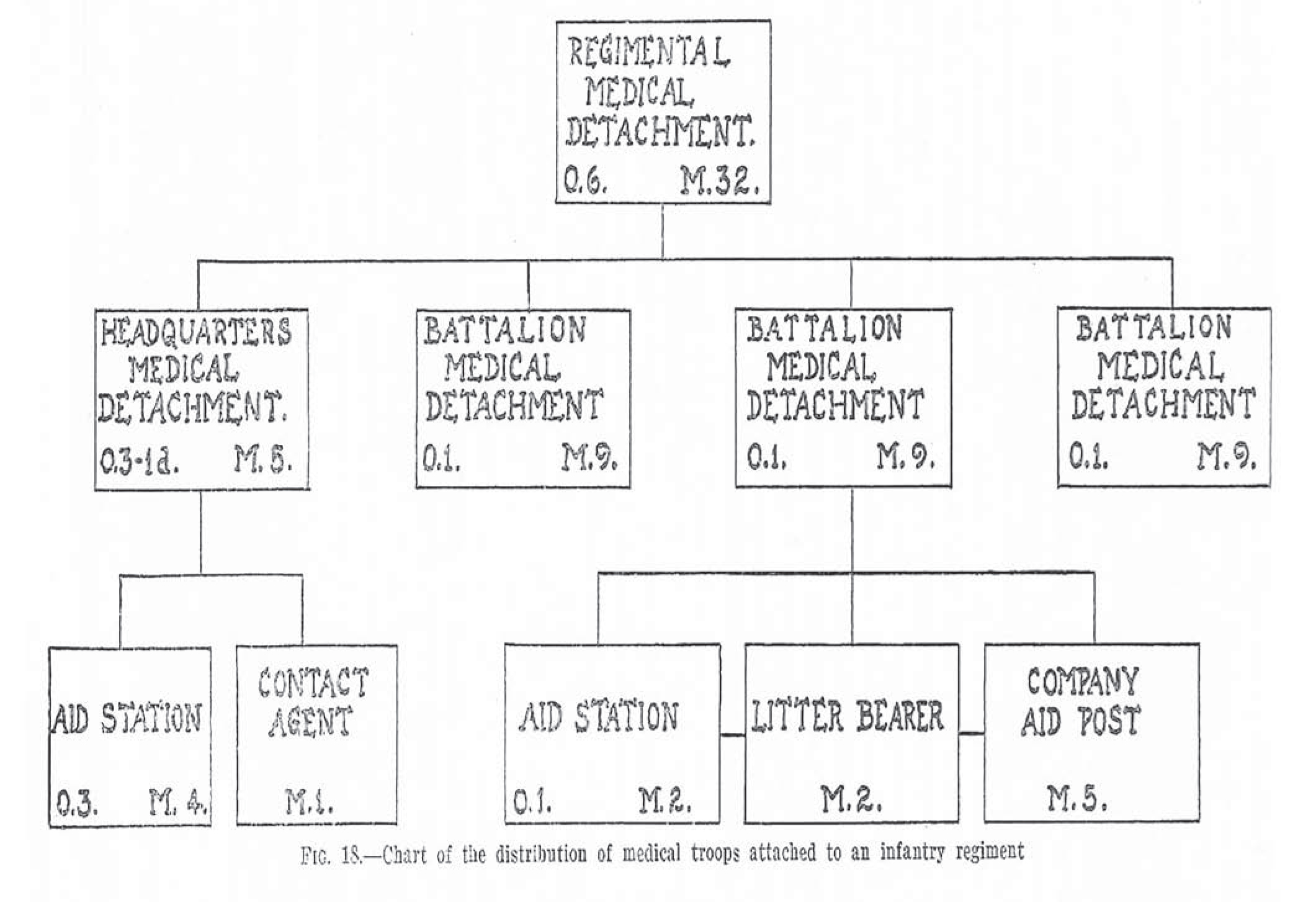
Medical plan for Marine infantry regiment. Adapted from LCdr William L. Mann, USN, Medical Tactics in Naval Warfare
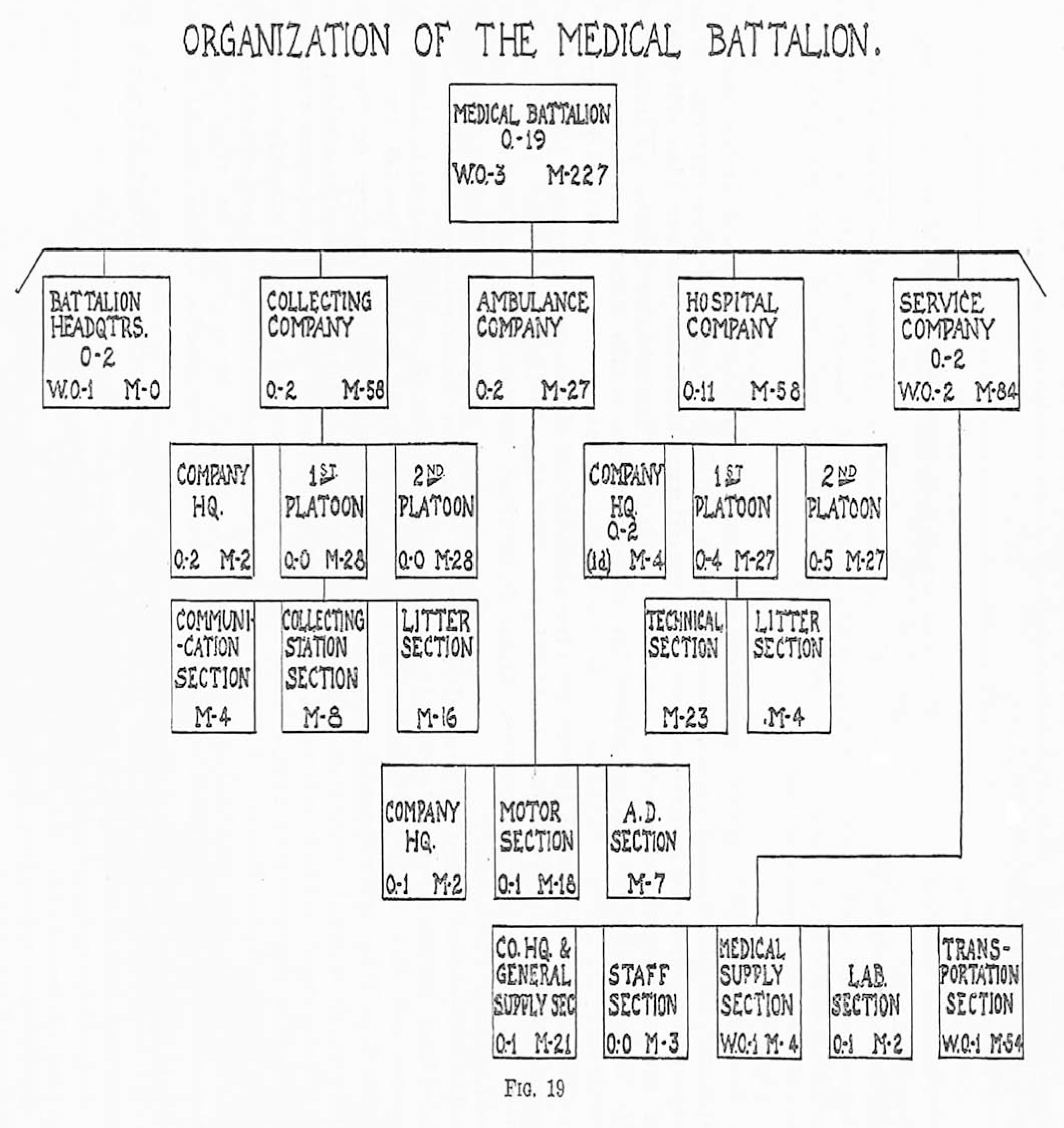
Adapted from LCdr William L. Mann, USN, Medical Tactics in Naval Warfare
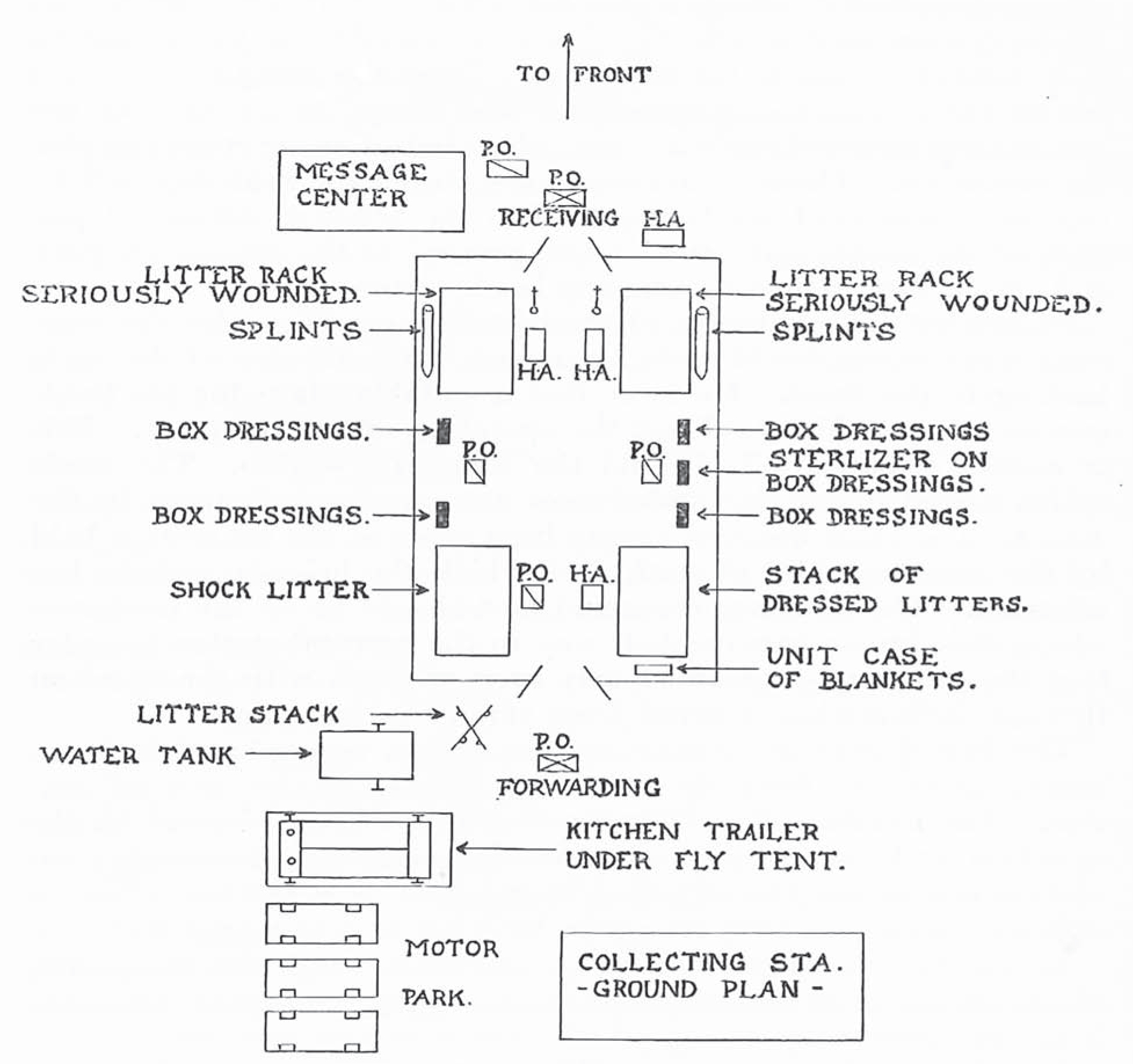
Adapted from LCdr William L. Mann, USN, Medical Tactics in Naval Warfare
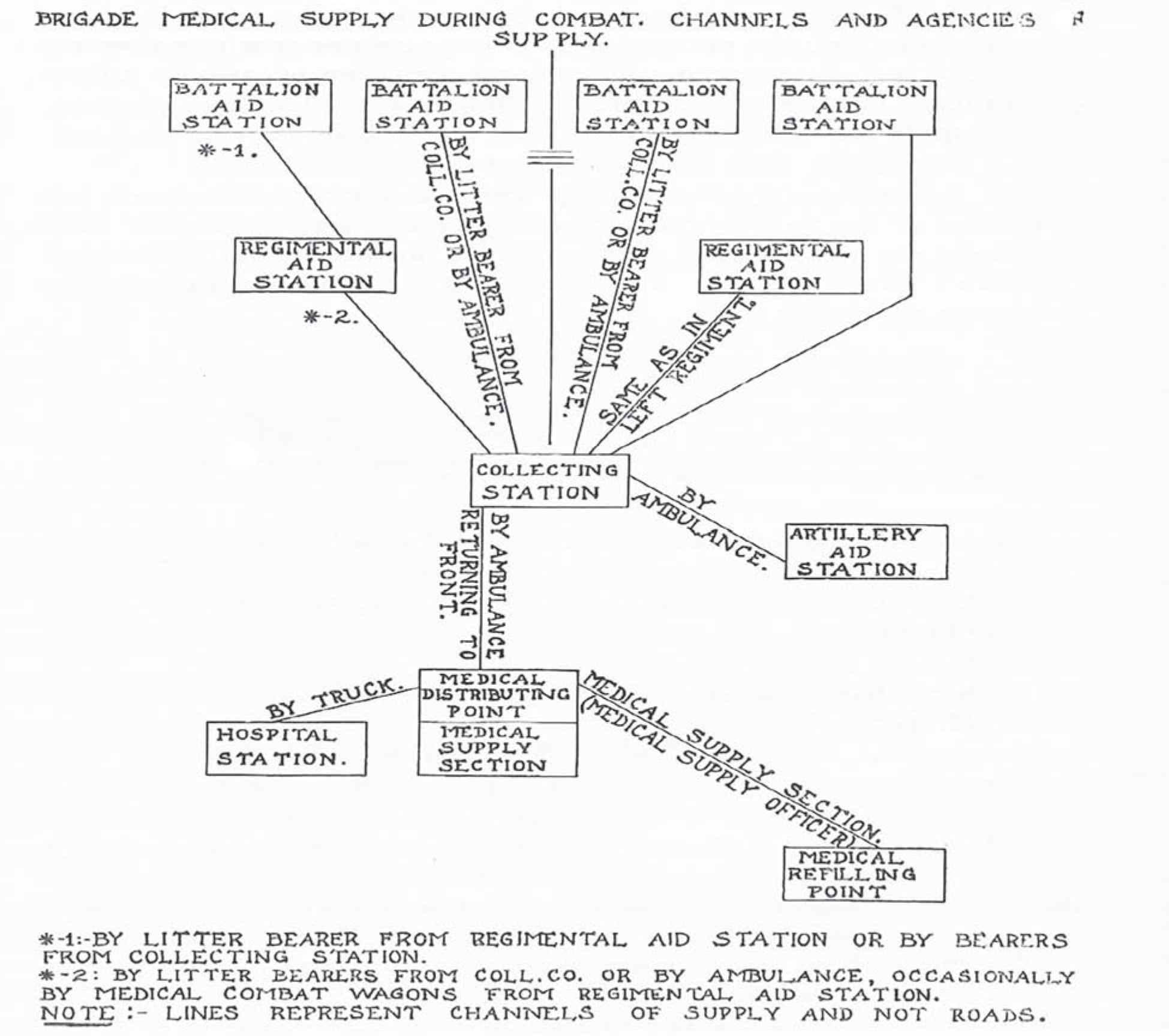
Brigade medical supply system. Adapted from Cdr William L. Mann, USN, Medical Tactics in Naval Warfare
These attempts to define medical support for the Marines in the early 1920s should be read in the context of the overall movement to transform the Marines and develop amphibious capability. Study of the British and Commonwealth assault on Gallipoli was considered essential to devising a workable doctrine for amphibious assault. Brigadier General Robert H. Dunlap, later Commandant of the Marine Corps, noted in his study of Gallipoli published in 1921, that pretty much everything had gone wrong.25 One of the five major areas that Brigadier General Dunlap highlighted as a failure was evacuation of the wounded, which had been a complete disaster. He noted specifically “evacuation of the wounded, requiring close cooperation between the Army and the Navy” was not performed properly.26
The Navy was also giving some consideration to the concepts of amphibious warfare, however, most of the Navy assumed that the Army would be involved in these operations, not the Marines. In a series of articles published in the U.S. Naval Institute Proceedings in 1924 and 1925 on Joint Army and Navy operations, Captain William S. Pye, USN, considered a wide range of issues. While the articles contained a great deal of detail on such subjects as properly fitting out of troop transports and conversion from standard merchant shipping, certain broad ideas applicable to development of a workable amphibious warfare doctrine were highlighted. These applied not only to overall conduct of amphibious operations, but also applied in terms of medical doctrine as well. Like General Dunlap, Captain Pye drew freely on the experience from Gallipoli and, in the first of his articles, he came out strongly in favor of prewar planning and practice between the Navy and the land component stating: “The British Army and Navy have been conducting joint operations for centuries yet the history of the Dardanelles Campaign, their latest large joint operation, indicates that almost every known error was committed at some time during the campaign.”27
Another lesson from Gallipoli that Pye highlighted was the need for unity of command, and he cited many examples (mostly from British experience) where the lack thereof led to disaster.28 Unity of command was not present in the medical aspects of the Gallipoli operation as well, where lack of a formal cooperative command structure resulted in major problems in both planning for and execution of medical treatment and casualty evacuation. In terms of the actual amphibious landing or assault, Captain Pye came to the conclusion that the process of landing troops still needed to be worked out.29
In an attempt to understand the workings of an amphibious assault, the Navy and Marines staged several landing exercises in 1922, 1923, and 1924 around the Caribbean at Culebra, Puerto Rico, and the Panama Canal Zone. The 1923 exercise was the first to include a medical component, although it was small. An aid station (of sorts) was established during the exercise, but it did not include casualty treatment. A more ambitious exercise was held by the Services in Hawaii in 1925.30 Not surprisingly, these exercises highlighted many shortcomings. The landing force was transported by the Navy on various warships from battleships to destroyers, which made shipboard conditions difficult for the Marines and created significant issues connecting troops with appropriate materiel. While the actual process of getting the Marines ashore improved from the complete shambles it was in 1922, all parties agreed that the use of standard crafts to land troops and supplies and to evacuate wounded from the beach was inadequate at best. Command and control of all sections represented another area of difficulty.
Unfortunately, the exercises in Hawaii in 1925 were to be the last of the 1920s. Commitments around the Caribbean and in China placed severe fiscal and personnel constraints on the Marines and on the medical personnel assigned to support them. There were neither the personnel nor the dollars available to devote to practicing amphibious landings or to individuals spending a great deal of “official” time working on solutions to the many problems highlighted during these exercises.
The Bureau of Medicine and Surgery, although very focused on the medical care of sailors ashore and aboard ship and various Navy operational issues, had not completely ignored the issues and needs of the Marines. The annual surgeon general’s reports to the secretary of the Navy for fiscal years 1924 and 1925 specifically mentioned, albeit briefly, medical operations with the Marines. In 1924, a report by Lieutenant Commander W. Chambers, Medical Corps, USN, on new equipment for use with the Marines was cited; and in 1925, the report stated “Considerable attention has been given to field service,” and the composition (personnel and equipment) of the medical battalion is described in detail, as were the courses of instruction at the schools at Quantico and the naval medical school for field service.31

Medical personnel set up an aid tent on San Clemente Island, California, during casualty movement training in the winter of 1937. U.S. Navy photo
While concentrated efforts in developing doctrine and techniques for amphibious operations were on a hiatus during the second half of the 1920s, some important developments took place. In 1927, the Joint Board of the Army and Navy formally gave the amphibious warfare mission to the Marines.32 The Joint Board served many of the same functions as the current Joint Chiefs of Staff does, one of which was to specify the roles and missions of each Service. The 1927 report defined the function of the Marines as follows:
10. (g) to establish and defend advanced naval bases.
11. (a): For land operations in support of the fleet for the initial seizure and defense of advanced bases and for such auxiliary land operations as are essential to the prosecution of the naval campaign.
VI 8 (b): Marine Forces: Marines organized as landing forces perform the same functions as above stated for the Army, and because of the constant association with naval units will be given special training in the conduct of landing.33
This Joint Board decision gave the Marines the green light to recast themselves as they had hoped to, including tasks they were to pursue vigorously once personnel and money became available.
Also in 1927, the Navy published Medical Tactics in Naval Warfare.34 This publication greatly expanded on the series of articles that Commander Mann had published the year prior in the United States Naval Medical Bulletin. The sections pertaining to medical support of amphibious operations and the Marines ashore represented the state-of-the-art concepts not only for U.S. forces but also for amphibious medicine around the world. While Mann’s article was as complete as anything in 1927, he recognized the limitations of the doctrine as it existed.
The first book on the tactics of landing operations has yet to be written . . . medical tactics connected with this type of military activity must conform and harmonize with the ideas of combatant branches . . . we have been compelled to follow closely, in the preparation of this study, the views outlined to us in informal conversations and discussions with the officers of the Army and Navy who have devoted considerable thought to landing tactics.35
Commander Mann had explained the need for Marine specific doctrine, training, and equipment, as distinct from the Army techniques, as follows:
The Naval Medical Department serving with the United States Marine Corps can pattern after and approach the Army medical organization and system of supplies, but unless the mission of the United States Marine Corps becomes identical with the mission of the United States Army, a difference in their two medical services must exist.36
In these two statements, Mann summarized the essence of the problems that faced naval medical officers in the coming years. First, that the organization and system (doctrine) for medical support of the Marine Corps must fit precisely with its mission, and secondly that, as of yet, the details of landing operation missions had not yet been defined. Thus, while lessons of the past could be studied to avoid making the same mistakes, and theoretical work could outline the “what” of medical amphibious doctrine, without well-developed tactics the medical department could make little progress in the “how” of medical doctrine.
Commander Mann then proceeded to present many of the issues that medical planners needed to tackle. He defined four types of Marine Corps operations that required medical support: naval landing parties, organized modern warfare, expeditionary service against semiorganized resistance, and occupation duty against semiorganized resistance.37 He outlined the different types of medical support for each type of operation, and the specifics of supply for each type of unit.38
Mann stressed the need for proper planning for medical aspects of an amphibious operation, particularly for the medical staff to constantly interface with line staff so as to be informed of important tactical considerations and casualty estimates. Like many other Navy and Marine Corps thinkers and planners Commander Mann used Gallipoli and the failures of coordinated planning there to illustrate his point. He also used a quote from Clausewitz’ On War that is almost a holy writ among planners: “In war everything must be simple, but the simple is usually difficult.” It is the natural tendency of the physician to concentrate on the sick or wounded patient in front of them, but the military medical planner has to raise their gaze beyond the individual patient. Because even the most junior doctor assigned to a Marine unit, the battalion surgeon, is by necessity a medical planner, Mann advised that “. . . in the field the distribution of medical supplies, prompt evacuation, skilled first aid, shelter, food, and restoratives available early for every fallen combatant are of infinitely more importance than highly technical relief to difficult cases.”39
Although unable to get into details for reasons already discussed, Mann did make important points with respect to concepts that had been disastrous at Gallipoli and problematic during the fleet landing exercises of the early 1920s, including medical regulation and loading supplies. He stressed that the medical team required adequate communications to keep track of the wounded and ensure that wounded would be sent to the appropriate locations.40 Anticipating the conclusions of the Marines who would deal with logistic and supply issues in the next decade, Commander Mann advocated collocating supplies for the medical unit on the same ship that carried medical personnel and ensuring that the most urgent medical supplies were loaded on top so they could be unloaded early in the assault.
Concepts such as combat loading and a proper system of medical regulation, as well as interfacing medical planners with line planners, might seem obvious in hindsight, but as Gallipoli and some of the difficulties in the fleet exercises of the 1920s illustrate, they were certainly not obvious, at least to those making decisions at the time. Although the successful German assault on the Baltic islands of Ösel, Moon, and Dagö was not studied until the early 1930s by American military analysts, it is worth noting that even with the lessons of Gallipoli to guide them, the Germans did not land any medical troops until 48 hours into the assault due to the low priority given them in loading and unloading. Because of the demoralized and disorganized conditions in the Russian Army on those islands and the rapid disintegration of most resistance, the German forces had very few casualties and thus avoided a disaster that might have been caused by poor medical planning.41 In addition to the more limited forces involved in direct Marine support, Commander Mann also discussed more capable but forward facilities. During the early part of a campaign, the plan was that hospital ships provided the most capable facilities (class A hospital ships). As the campaign advanced and a significant secure area acquired, tent-based “base hospitals” of 500 beds, expandable to 1,000 beds, were to be established.42 Other sections of Mann’s book dealt with specific shipboard issues, and sanitation and other measures that would fall under the general heading of preventative medicine.
As the 1920s drew to a close, much had been accomplished by amphibious planners, but much was yet to be done. Not only had the Marines decided to transform and become centered around amphibious operations, but the 1927 Joint Board decision had ratified that decision and awarded the Marines that niche within the U.S. military establishment. From the medical side, such pioneers as Commander Mann had already begun serious analysis of the difficulties of medical support for amphibious operations, and had outlined many of the major concerns and had begun to take steps to find solutions. However, absent an overall doctrine for amphibious operations, as well as technical solutions to such problems as adequate landing craft, medical planners could only go so far in their doctrinal designs. Navy and Marine Corps resources were stretched too thin by operational commitments to continue the fleet landing exercises into the second half of the 1920s, robbing the forces of the opportunity to experiment and gain experience.

During casualty movement training (1937), stokes litters are shown transporting casualties. U.S. Navy photo
Most importantly, a small group of naval medical officers led by Commander Mann and Lieutenant Commander W. A. Vogelsang had made an important start. They had properly identified that medical support for amphibious operations was not the same as medical support for a more “normal” land campaign. Having identified that there was a problem, and a huge gap in doctrine, they had begun to define the individual elements that made up the whole. In fact, the base laid down in the 1920s for defining the outlines of medical doctrine for amphibious operations proved remarkably prescient. Fortunately for Marines, Commander Mann, Lieutenant Commander Vogelsang, Captain Chambers, and others continued to be involved in the development of medical doctrine for amphibious operations.
The close of the decade would usher in both challenges and opportunities for the Marine Corps and the Navy physicians who supported them. The Great Depression would only add to the financial stringencies that all of the armed Services struggled with. At the same time, the marked reduction in overseas commitments of the Marines in the Caribbean and Central America would free up resources for other purposes. As you will see in part two of this discussion, the early 1930s would see an emphasis on the development of Marine Corps doctrine for amphibious warfare, the search for adequate landing craft, and the realization by a small group of Navy physicians of the need for the development of a scheme of medical support to complement this doctrine.